


IVF and Endometrial Biopsy: Why Sampling the Lining Matters
The endometrium is the inner lining of the uterus where embryo implantation must occur, and its biological state at the moment of transfer is one of the most critical determinants of whether an IVF cycle succeeds or fails. While transvaginal ultrasound provides valuable information about endometrial thickness and pattern, it captures only the structural surface of what is fundamentally a molecular and cellular phenomenon. Endometrial biopsy provides direct access to the tissue itself, allowing the analysis of cellular populations, genetic expression patterns, microbial communities, and pathological conditions that ultrasound cannot detect.
Understanding what endometrial biopsy tests for, when it is most clearly indicated in IVF planning, what different biopsy results mean for subsequent treatment, and what the procedure involves from the patient's perspective gives couples a more complete appreciation of one of the most clinically productive investigations available for addressing unexplained implantation failure.
What Endometrial Biopsy Involves
An endometrial biopsy is a minimally invasive outpatient procedure in which a small sample of endometrial tissue is collected from the uterine cavity using a thin catheter or sampling device passed through the cervix. The procedure is performed without general anaesthesia in most cases and takes approximately five to ten minutes.
Most patients experience mild to moderate cramping during the sampling, comparable in character to menstrual cramping, that typically resolves within minutes to hours after the procedure. Some bleeding and spotting for one to two days following the biopsy is normal and expected.
The tissue sample is then processed according to the specific test being conducted. Different investigations require different processing approaches, from standard haematoxylin and eosin staining for histological assessment to immunohistochemistry for specific cell markers to next-generation sequencing for microbiome or gene expression analysis. Ensuring that the sample is collected and processed correctly for the specific test intended is an important quality step that experienced fertility laboratories manage systematically.
Testing for Chronic Endometritis
Chronic endometritis is the most commonly sought diagnosis in endometrial biopsy conducted as part of a recurrent implantation failure investigation. As discussed in the endometrial receptivity guide in this series, chronic endometritis is a low-grade bacterial infection of the uterine lining that impairs receptivity through local inflammatory disruption without producing the obvious symptoms that would prompt investigation in the absence of a specific search.
The diagnosis is made through immunohistochemistry staining for CD138, a surface marker specifically expressed on plasma cells but not normally present in the endometrium. The presence of plasma cells infiltrating the endometrial stroma, identified as CD138-positive cells on immunostained biopsy sections, is the diagnostic criterion for chronic endometritis.
Research has found chronic endometritis in a meaningful proportion of women with recurrent implantation failure who had not been previously diagnosed or treated for the condition. Treatment with a targeted antibiotic course based on endometrial culture results, confirmed by repeat biopsy showing resolution, has been associated with improved subsequent IVF outcomes in multiple clinical series.
The Endometrial Receptivity Assay
The endometrial receptivity assay is a specific genetic test conducted on endometrial biopsy tissue that analyses the expression of a panel of approximately two hundred genes to classify the endometrial sample as receptive, pre-receptive, or post-receptive at the time of biopsy.
The ERA test is conducted in a mock transfer cycle in which the patient's uterine lining is prepared with the same hormonal protocol planned for her actual embryo transfer. Biopsy is taken at the time when the standard protocol would schedule the transfer, and the gene expression profile of the sample is compared against a reference database to determine whether the endometrium is in the receptive state at that timing.
If the biopsy is classified as receptive, the standard transfer timing is confirmed. If it is pre-receptive, the endometrium had not yet reached peak receptivity at the standard timing and progesterone should be extended by a specified number of hours or days. If it is post-receptive, the window has already passed and progesterone should be shortened. Transfer timing in the subsequent real cycle is then adjusted based on these results, a concept called personalised embryo transfer.
The ERA test has its strongest evidence base in patients with repeated implantation failure despite good embryo quality and an apparently normal uterine cavity where other causes of failure have been excluded. In this specific population, a displaced implantation window has been identified in a clinically significant proportion of patients and correction of transfer timing has shown improved subsequent outcomes in several studies.
Endometrial Microbiome Testing
As discussed in the endometrial microbiome guide in this series, next-generation sequencing of endometrial biopsy samples can assess the microbial community within the uterine cavity and determine whether the Lactobacillus-dominant profile associated with better IVF outcomes is present or whether a non-Lactobacillus-dominant dysbiosis that may impair implantation predominates.
Endometrial microbiome testing from biopsy samples provides more direct information about the uterine microbial environment than vaginal swab-based microbiome testing, because the vaginal and uterine microbiomes are related but not identical. A non-Lactobacillus-dominant uterine microbiome identified on endometrial biopsy may be addressed through targeted probiotic supplementation or, where specific pathogenic bacteria are identified, targeted antibiotic treatment followed by probiotic restoration.
Histological Assessment for Endometrial Development
Standard histological assessment of endometrial biopsy has been used for decades to determine whether the endometrium is in the appropriate secretory phase for its cycle day, a concept historically called endometrial dating. An endometrium that is out of phase with the expected cycle day based on its histological appearance has been proposed as a marker of endometrial receptivity dysfunction.
The clinical utility of histological endometrial dating for predicting IVF outcomes has been questioned by research finding poor reproducibility of dating criteria between pathologists and poor correlation between dating results and clinical outcomes. Most contemporary reproductive medicine guidelines do not recommend standard histological endometrial dating as a primary investigation for implantation failure, having been largely superseded by the ERA test for receptivity assessment.
However, standard histology remains clinically useful for identifying specific endometrial pathologies including glandular abnormalities, stromal decidualisation defects, and in conjunction with immunohistochemistry, the plasma cell infiltration of chronic endometritis. The biopsy sample therefore serves multiple investigative purposes when processed appropriately.
When Endometrial Biopsy Is Most Clearly Indicated
Endometrial biopsy is most clearly indicated in several specific clinical scenarios within IVF planning.
Recurrent implantation failure, defined as two or more failed transfers of good quality embryos with an apparently normal uterine cavity on standard assessment, is the strongest indication for endometrial biopsy. The combined assessment for chronic endometritis, displaced window of implantation through ERA testing, and endometrial microbiome profiling covers the most important and most clinically actionable factors that endometrial biopsy can identify in this population.
Unexplained recurrent pregnancy loss, where embryo chromosomal causes have been addressed through PGT-A and uterine structural causes have been excluded through hysteroscopy, represents another indication for endometrial biopsy investigation of the implantation environment.
Specific clinical features including a history of pelvic inflammatory disease, previous instrumentation of the uterine cavity, irregular or abnormal uterine bleeding, or clinical features suggesting endometritis warrant endometrial assessment before IVF even in patients approaching their first cycle.
Connecting with an experienced Best IVF Center in Sikar that performs endometrial biopsy with appropriate timing, processes samples for the specific investigations most relevant to each patient's clinical situation, and integrates biopsy findings into a modified and targeted treatment plan ensures that this clinically productive investigation is applied with the precision and clinical purpose that maximises its diagnostic yield for your specific situation.
Final Thoughts
The endometrium is the site of one of the most complex and most consequential biological events in human reproduction. Endometrial biopsy provides direct access to the tissue at the heart of that event and allows investigations of its cellular, microbial, and molecular state that no surface assessment can match.
For patients with unexplained implantation failure, it is often where the answers are. For patients approaching a first IVF cycle with specific risk factors for endometrial dysfunction, it is where the preventable contributors to failure are most directly identified.
For expert endometrial assessment combining biopsy-based investigations with the full range of ERA, microbiome, chronic endometritis and histological analysis appropriate to each patient's clinical situation, a trusted ivf clinic in jaipur with access to the most informative endometrial investigations and the clinical expertise to integrate their findings into individualised treatment planning gives your uterine preparation the most thoroughly characterised foundation available.
Disclaimer: This article is intended for informational purposes only and does not constitute medical advice. Please consult a qualified fertility specialist for guidance tailored to your individual diagnosis and treatment needs.
Κατηγορίες
Διαβάζω περισσότερα
Las casas de apuestas España han experimentado una notable evolución durante los últimos años, convirtiéndose en una de las principales opciones de entretenimiento para miles de aficionados al deporte y a las predicciones de resultados. Gracias al desarrollo tecnológico y a la creciente digitalización de los servicios, los usuarios...

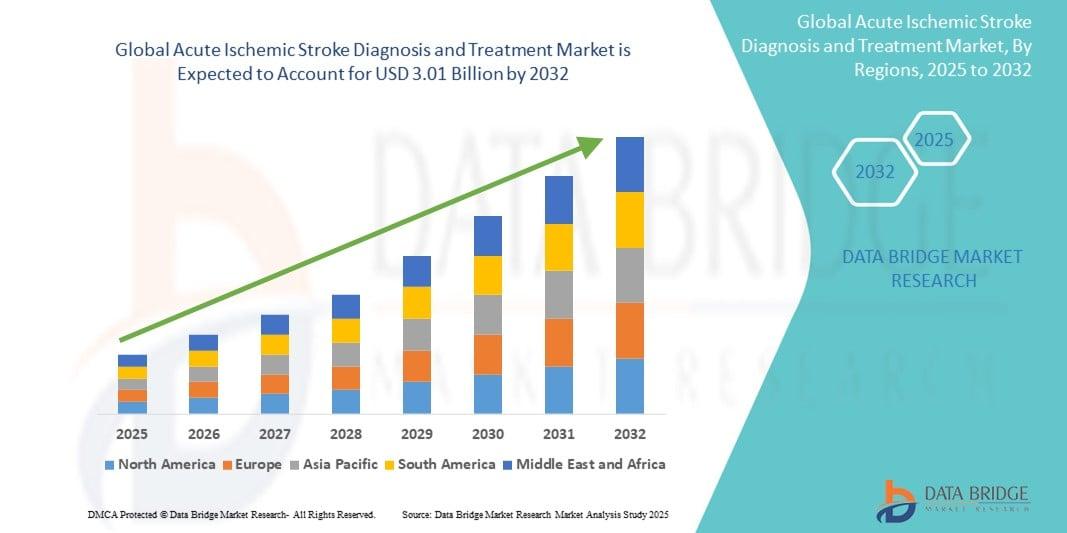
"Acute Ischemic Stroke Diagnosis and Treatment Market Summary: According to the latest report published by Data Bridge Market Research, the Acute Ischemic Stroke Diagnosis and Treatment Market The global acute ischemic stroke diagnosis and treatment market size was valued at USD 1.79 billion in 2024 and is expected to reach USD 3.01 billion by 2032, at a CAGR...
The U.S. Medical Examination Lights Market is witnessing steady growth as healthcare providers increasingly invest in advanced illumination systems to improve diagnostic accuracy, patient safety, and clinical efficiency. Rising demand for minimally invasive procedures, expansion of outpatient care facilities, and ongoing modernization of healthcare infrastructure are creating significant...

Let us be honest—everyone loves a good deal. There is a genuine satisfaction in finding quality service at a price that respects your budget. But when it comes to carpet cleaning, the pursuit of savings can sometimes lead homeowners down a risky path. Too often, the cheapest quote comes with hidden fees, rushed work, or disappointing results that leave carpets wet for days or stains...

In today’s competitive academic environment, students need more than classroom learning to excel in their studies. CBSE online tuition has emerged as a reliable and effective solution for students who want personalized guidance, flexible learning, and expert support. With live online classes conducted by experienced tutors, students from Classes 1 to 12 can strengthen their understanding...
