


Documenting "Hospital-in-the-Home" Remote Vitals Integration

The healthcare industry is currently witnessing a paradigm shift with the rapid expansion of "Hospital-in-the-Home" (HiTH) programs. This model allows patients to receive acute-level care in the comfort of their own residences, supported by a network of clinicians and sophisticated monitoring technology. However, the success of HiTH depends heavily on the seamless integration of remote vitals into the patient’s permanent medical record. Unlike traditional hospital settings where vitals are recorded at the bedside by nursing staff, remote vitals often arrive as a digital stream of data or via voice-recorded updates from visiting clinicians. Ensuring that this information is transcribed and documented with 100% accuracy is vital for clinical decision-making. The transition from digital data to a narrative medical history requires a high level of administrative precision to ensure that subtle trends in a patient’s recovery are not lost in translation.
The Role of Accurate Transcription in Remote Patient Monitoring
In a remote care environment, clinicians often use dictation tools to record their observations and the nuances of a patient’s condition during home visits. This recorded data must be converted into text and integrated into the Electronic Health Record (EHR) with extreme speed. Any delay or error in this process can lead to a misunderstanding of the patient's physiological status. For administrative professionals working in these high-stakes environments, having a foundation from an audio typing course is indispensable. It ensures that the speed of documentation matches the real-time nature of remote monitoring. High-speed, accurate transcription allows the "Hospital-in-the-Home" model to function as a cohesive unit, where the remote data and the clinician’s narrative work together to provide a comprehensive view of the patient’s progress without the need for physical hospital occupancy.
Challenges of Integrating Disparate Data Streams
One of the primary hurdles in documenting HiTH vitals is the lack of standardization across different remote monitoring devices. While one device may automatically upload heart rate data, a visiting therapist might dictate blood pressure readings and oxygen saturation levels during a home visit. This creates a fragmented record that must be unified by a skilled medical secretary or administrator. The ability to listen to complex clinical terminology and transcribe it accurately is a skill that is heavily emphasized in a professional audio typing course. These specialists are trained to handle the varied accents, background noises, and technical jargon that are common in home-based recordings. By converting these disparate voice recordings into a standardized textual format, they provide the "connective tissue" that allows various specialists to review the same data set and collaborate on the patient’s treatment plan regardless of their physical location.
Enhancing Clinical Safety Through Narrative Documentation
While automated data alerts are useful for flagging immediate emergencies, the narrative documentation provided by clinicians is what provides context to the numbers. For instance, a spike in heart rate might be concerning on a monitor, but a dictated note explaining that the patient was performing prescribed physical therapy provides necessary context. For this reason, the transcription of clinical notes must be handled with a level of care that automated software often lacks. Enrolling in an audio typing course prepares administrative staff to recognize the critical importance of punctuation and medical context, which can change the meaning of a clinical observation if handled incorrectly. In the "Hospital-in-the-Home" model, where the physician may not see the patient in person for several days, these transcribed notes become the primary tool for maintaining patient safety and ensuring that the remote care plan is being followed correctly.
Ethical and Legal Implications of Remote Documentation
As more sensitive health data is recorded and transcribed outside of traditional hospital walls, the legal and ethical responsibilities surrounding documentation have increased. HiTH programs are subject to the same rigorous HIPAA or GDPR standards as traditional hospitals, meaning that the transcription process must be secure and the resulting records must be beyond reproach. Errors in transcription can lead to serious legal liabilities for a healthcare provider. Professionals who have polished their skills through an audio typing course are taught the importance of confidentiality and the high standards required for legal medical documentation. This professional background ensures that the hospital-at-home program remains compliant with national health regulations while providing a robust defense in the event of an audit or a legal inquiry regarding the quality of care provided in the patient’s residence.
Future Outlook: The Synergy of AI and Human Expertise
The future of documenting remote vitals likely involves a hybrid approach where Artificial Intelligence handles the initial data sort, and human experts provide the final, verified transcription. AI still struggles with the nuances of clinical judgment and the varied acoustic environments of home-based care. Therefore, the demand for human transcribers who have completed an audio typing course remains high. These individuals serve as the final quality control layer, ensuring that the AI has not misinterpreted a critical value or a specific clinical instruction.
Kategoriler
Read More
AI is everywhere in business conversations today. But many companies are still asking the same question: How do we turn AI into real business growth? Organizations often experiment with automation tools, predictive models, and analytics platforms, yet these initiatives rarely move beyond small pilot projects. AI transformation services help businesses integrate artificial intelligence into real...

"Above Ground Pools Market Summary: According to the latest report published by Data Bridge Market Research, the Above Ground Pools Market The global above ground pools market size was valued at USD 3.26 billion in 2024 and is expected to reach USD 4.86 billion by 2032, at a CAGR of 5.10% during the forecast period The universal Above Ground Pools Market...
Long days in New York can leave anyone feeling drained. At Garden Retreat Spa, we provide Nomad Massage New York treatments to help restore your energy and relieve stress. Our team uses a combination of gentle and targeted techniques that ease tension and improve circulation. Whether it’s your first visit or a regular escape, we make sure each session leaves you feeling lighter and...
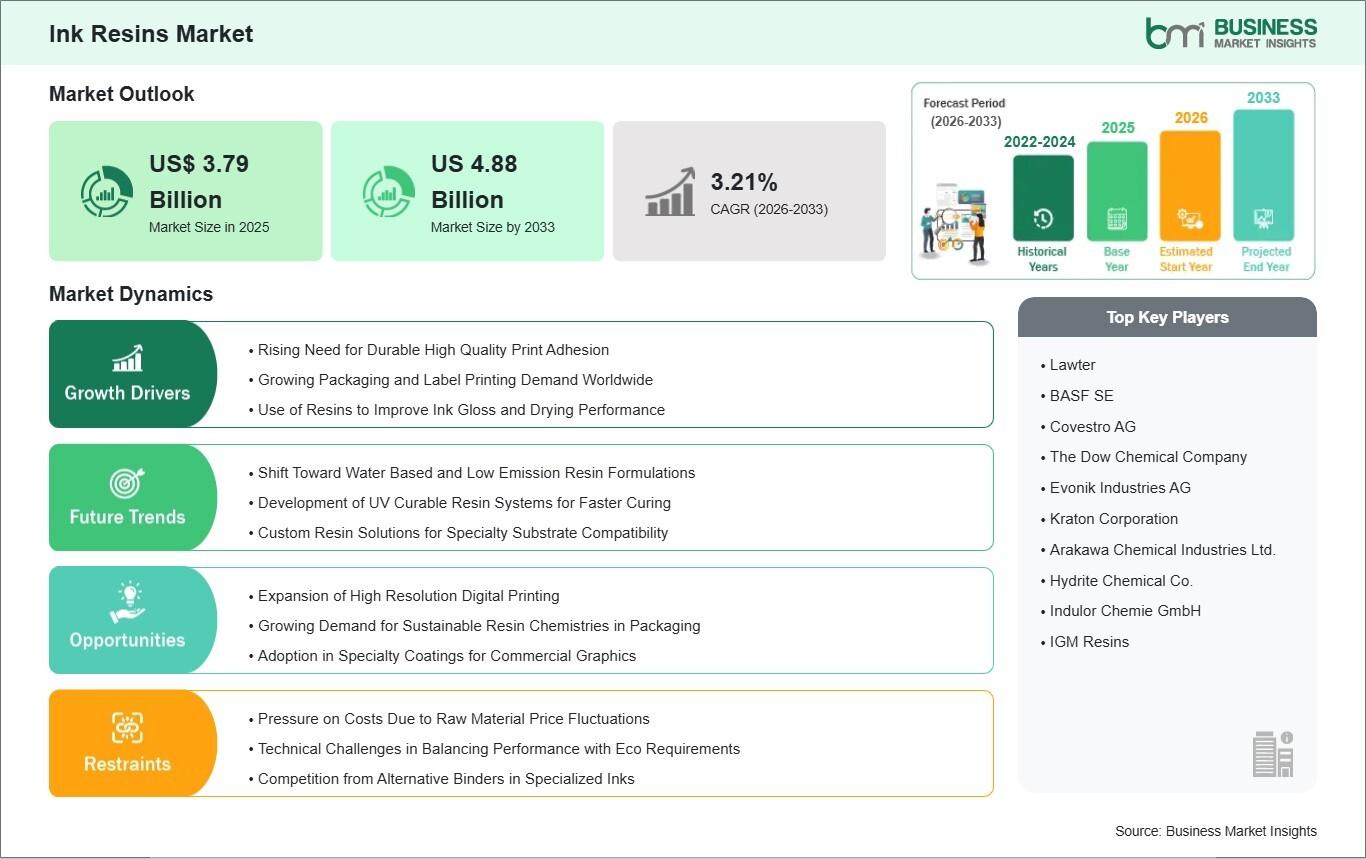
Driven by shifting consumer preferences, the explosive growth of e-commerce, and stringent international environmental regulations, the global printing and packaging industries are experiencing a profound technological transformation. Data published by Business Market Insights indicates that the international Ink Resins Market will grow at a CAGR of 3.21% from 2026 to 2033, scaling its overall...
Security has become a top priority for businesses of every size. Whether managing a corporate office, healthcare facility, educational institution, warehouse, or commercial property, organizations need reliable solutions that protect people, assets, and sensitive information. Traditional lock-and-key methods are no longer sufficient for modern security challenges. This is where a quality access...
